
What is Down syndrome?
Down syndrome is one of the most common genetic variations and occurs in approximately one in every 700 live births in the United States. For most people, each cell in the body has 23 pairs of chromosomes. One chromosome in each pair comes from the mother and the other comes from the father. But sometimes, during cell division, an extra copy of the 21st chromosome is present. As the cells multiply and the pregnancy is carried to term, a baby with Down syndrome is born.
What causes Down syndrome?
Scientists have investigated the causes of Down syndrome for the past century. So far, its exact cause has eluded discovery. Doctors aren’t sure why this happens. There’s no link to any environmental factors or anything the parents did or didn’t do. Although many factors have been considered possible causes, the mother’s age is the most often discussed factor related to the likelihood of having a baby with Down syndrome because older eggs have a greater risk of improper chromosome division. It has been known for some time that the risk of having a child with Down syndrome increases with the mother’s advancing age. For instance, the risk of a 20-year-old mother giving birth to a child with Down syndrome is about 1 in 1600, the risk at age 35 is 1 in 365, and the risk at age 40 increases to 1 in 100. However, the majority of babies with Down syndrome are born to mothers less than 35 years old. This is because there are many more births among younger women.
Are there different types of Down syndrome?
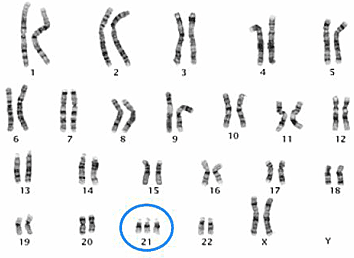
According to the CDC, there are three types of Down syndrome: Trisomy 21, Translocation Down syndrome, and Mosaic Down syndrome. The difference between each type can only be determined by looking at the chromosomes under a microscope as the physical features and behaviors are similar.
Trisomy 21: About 95% of people with Down syndrome have Trisomy 21. In this type of Down syndrome, each cell in the body has three separate copies of chromosome 21 instead of the usual two copies.
Translocation Down syndrome: This type accounts for about 3% of people with Down syndrome. It occurs when an extra part or a whole extra chromosome 21 is present, but it is attached or “trans-located” to a different chromosome rather than being a separate chromosome 21.
Mosaic Down syndrome: This type affects about 2% of the people with Down syndrome. Mosaic means mixture or combination. For children with mosaic Down syndrome, some of their cells have three copies of chromosome 21, but other cells have the typical two copies of chromosome 21. Children with Mosaic Down syndrome may have the same features as other children with Down syndrome. However, they may have fewer characteristics of the condition due to the presence of some (or many) cells with a typical number of chromosomes.
What are the physical characteristics of Down syndrome?
There are various common physical features among babies with Down syndrome. Not every baby born with Down syndrome will possess each of the characteristics. Many characteristics most commonly associated with Down syndrome can also be found in the general population. Some more noticeable common physical features found in babies with Down syndrome include:
- Low muscle tone (hypotonia) which makes muscles appear relaxed or “floppy”
- Loose joints
- Almond-shaped upward slanting eyes
- A flattened face and/or nose bridge
- Smaller ears, hands, and/or feet
- Small pinky fingers that sometimes curve toward the thumb
- A single crease across the palm of the hand (palmar crease)
- A deep groove between the first and second toes
- A short neck
- A protruding or larger tongue
- Tiny white spots on the colored part of the eye (Brushfield spots)
It should be noted that there is no correlation between the number of characteristic features a baby has and the child’s cognitive ability.
Can Down syndrome be treated or cured?
Down syndrome is a lifelong condition. Although it cannot be cured, medical professionals know more about it now than ever. Getting the best care early on can make a big difference for individuals with Down syndrome and improves the likelihood of a full and meaningful life.
How will having Down syndrome affect my baby?
Babies born with Down syndrome will grow and develop like all the other babies, but those with Down syndrome generally develop at a somewhat slower pace. Children with Down syndrome may be delayed in achieving milestones such as walking, talking, and eating compared to typically developing children. Children who have Down syndrome may also face intellectual and behavioral delays. Having a loving home environment and early intervention and special education services will positively influence a child’s development in all areas.
What is the life expectancy of people with Down syndrome?
Over the years, medical research, technology, and practices have helped prolong individuals with Down syndrome’s life span. Today the majority of individuals will live upwards of age 60 or 70.
-
NDSC Down Syndrome Information
-
Prenatal & Newborn Information
National Down Syndrome Congress, GLOBAL Down Syndrome Foundation, and National Down Syndrome Society have teamed up to publish the second edition of the groundbreaking Prenatal & Newborn Information Pamphlet, available in English, Spanish and Icelandic. The second edition, created from the first national survey of pregnant women and medical professionals, is easily accessible electronically, or in print at no cost.
Prenatal & Newborn Information Pamphlet – English
If you would like to discuss any aspect of what is offered here, please call the NDSC Center, toll-free, at 1-800-232-NDSC (6372), Monday through Friday from 9:00 AM to 5:30 PM eastern time.